Short implants are currently experiencing a huge wave of commercial and clinical interest, with large implant companies like Nobel Biocare, Straumann, Dentsply Sirona, Biohorizon, and Zimmer Biomet all introducing their own offerings in recent years. Defined as implants with a designed intrabony length (DIL) equal to or less than 8 mm, short implants once occupied the far fringe of the implant market. Their recent rise to the mainstream may give some clinicians the false impression that these lengths of implants are new and relatively untested, but in reality, science established the value of short implants much earlier than the market did. Dr Douglas Deporter, a clinician and researcher who has devoted more than 30 years to the clinical study of short and ultra-short implants and who is the editor of a book on the topic, reflects on why he has dedicated his career to short implants. He also explains why their surge in clinical prominence today is wholly deserved.
A Periodontist’s Path to Implant Dentistry
“My interest in dental implants started almost 40 years ago,” explains Douglas Deporter, DDS, Dip Perio, PhD. “In 1979, I was a newly appointed assistant professor at the University of Toronto (U of T). The head of prosthodontics at my faculty, Prof George A. Zarb, proposed a site visit to investigate firsthand the rumors that an orthopedic surgeon by the name of Per-Ingvar Brånemark and his colleagues in Göteborg, Sweden, had developed and were testing a pure titanium threaded dental implant for tooth replacement. I was asked to be a member of the site visit team, and hence began my involvement in the implant field. Prof Zarb later organized a replication trial of Brånemark implants at U of T called ‘The Toronto Study.’ The early findings from The Toronto Study were supportive enough by 1982 that Prof Zarb and the Brånemark camp organized the first meeting in North America dedicated to the Brånemark implant concept, called the Toronto Conference on Osseointegration in Clinical Dentistry.”
My colleagues and I were thought to be way off base in thinking that implants could be much shorter in length than the standard lengths.
The invitation-only Toronto meeting primarily included prosthodontists and oral surgeons. Interestingly enough, periodontists were originally excluded from implant research and treatment due to the early opinion that the quality and quantity of soft tissue around implants was irrelevant. However, Dr Deporter managed to attend the Toronto meeting, and the experience changed his career path as a periodontist.
“I attended the Toronto conference with several members of our faculty,” Dr Deporter recalls, “including Prof Robert M. Pilliar, a biomaterials scientist responsible for the development of a highly successful cementless hip implant prosthetic device. Bob was intrigued by the idea of titanium dental implants, but not those like the Brånemark implant, which was a smooth machine-surfaced threaded device. Instead, he suggested to us that the same surface technology from his hip implant, which had a sintered porous surface (SPS) topography, could be applicable to dental implants and may offer some unique advantages over the threaded screw concept.”
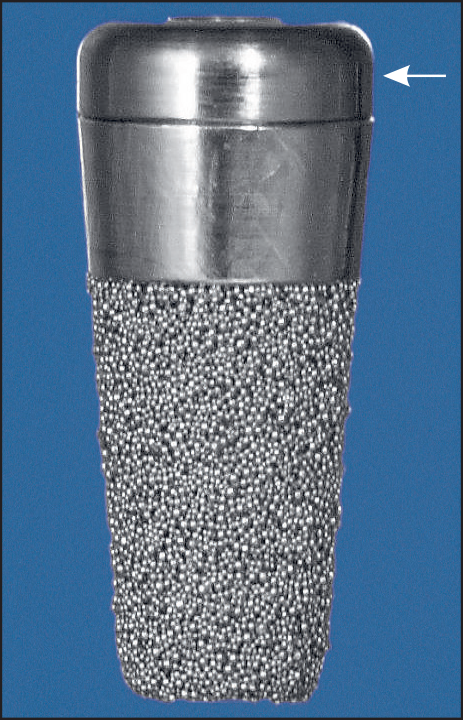
The 7-mm-long SPSI Dr Deporter and his colleagues designed (Endopore, Innova Life Sciences) with healing cap (arrow). The DIL was only 5 mm because there was a 2-mm machine-turned collar segment. This size implant had a 20-year absolute survival rate of 90% when used to retain mandibular complete overdentures.
The SPS implant that Dr Deporter and his colleagues designed and tested was fabricated from titanium alloy and had a 5-degree taper to make it similar in shape to natural tooth roots. Early animal experiments indicated that the team was on the right track: They found that the sintered surface provided a much stronger bone-to-implant interface than a threaded implant with a machine-turned surface. The University of Toronto obtained a patent for the implant and awarded a license to Innova LifeSciences to produce it. Innova subsequently applied for approval from the US Food and Drug Administration (FDA).
“As expected, the FDA expressed doubt about the short implant lengths being used,” Dr Deporter recalls. “They insisted that our clinical work be duplicated by a small group of American dentists on American patients. The American clinicians, however, wanted longer implant lengths available to use when bone height allowed them to be used. Frankly, they did not believe that our short implant could work. In order to fulfill their request, Innova produced a 12-mm-long version, 12 mm being the maximum length possible with the implant’s designed 5-degree taper angle. We tried out some of these longer ones at U of T as well and, along with the US investigators, concluded that the longer length was of no advantage and may even underperform compared with our standard shorter length.”
Early Resistance
While the Toronto meeting galvanized interest in dental implants, it did so only for one type of dental implant—the Brånemark threaded implant—and only at lengths between 10 and 20 mm. Few in the dental community were as adventurous and willing to stray from the Brånemark path as Dr Deporter and his colleagues were. Further obstructing the acceptance of short implants were problems arising from early study designs and the way their results were presented, which unfortunately became the foundation of opinion for most clinicians and researchers.
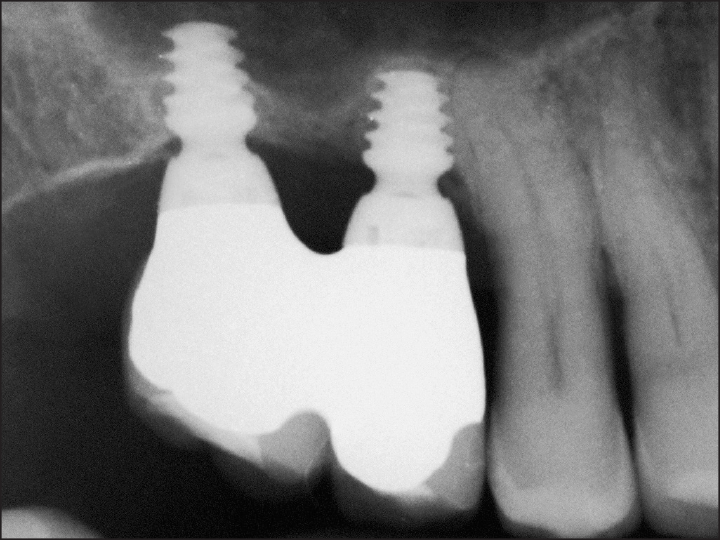
Radiograph of two 4 × 4–mm ultra-short moderately rough threaded implants after 1 year in function in the posterior maxilla. (Courtesy of Dr Pietro Felice, University of Bologna, Italy; restoration by Dr Michele Diazzi, Bologna, Italy.)
“My colleagues and I were thought from the outset to be way off base in thinking that implants could be much shorter in length than were then seen to be safe and predictable,” Dr Deporter explains. “General opinion at the time was that if Brånemark implants were available in lengths ≥ 20 mm, how could an SPS implant with a DIL of just 5 mm work equally well? The conclusion was introduced that short lengths were inappropriate for Brånemark-type implants following early applications by less experienced clinicians such as those participating in The Toronto Study. However, later research verified that short Brånemark-type implants could have high survival rates even in the posterior maxilla as long as appropriate surgical modifications were made to the placement techniques.”
Once short implants have been fully integrated in bone, they behave just like longer implants.

(a) Scanning electron microscope (SEM) of a particle-blasted, acid-treated moderately rough threaded implant surface (original magnification ×2000). (b) SEM of an SPSI surface (original magnification ×200). (c) SEM of an SPSI surface after pull-out from a healed implanted site in a rabbit femur. Extensive bone ingrowth can be seen at the sheared bone-to-implant interface surface (original magnification ×300).
The first implants developed and tested successfully by Brånemark were under 8 mm in length.
One of the most important tenets of scientific research is to compare ‘apples to apples’ when comparing two things. It’s why controls are an important part of study design. Clinicians in these early studies were applying short implants in less favorable conditions than standard-length implants, but they weren’t controlling the reported data to accommodate those differences. This resulted in misleading comparisons between the efficacy of short versus standard-length implants. Hindsight and modern research also allow for the observation that the less-than-ideal machine-turned surface of early implant designs could have had a far more negative impact on outcomes than implant length.

This radiograph shows the status of two ultra-short implants after 2 years in function in
the resorbed posterior mandible. Note the increase in bone density adjacent to and between the two implants. Crestal bone has crept over the implant shoulders toward the neck segment.
“In 2005,” Dr Renouard states, “Hermann et al analyzed a large number of failed implant procedures and reported that short implants had usually been used in sites with low bone volume and density, whereas longer implants were nearly always placed in denser bone. This observation challenges implant length as the cause of failure. For example, did an implant in the posterior maxilla fail because of its length, or was the result caused by low bone density and the clinician’s failure to appropriately modify osteotomy preparation?”
The misleading presentation of success rates with short implants can be partially excused by simply not knowing then what we know now about important factors of success for endosseous implants. It can also be attributed in part to a phenomenon affecting all areas of research.
“The adaptation of these findings to comply with the general consensus at the time (ie, that implants shorter than 10 mm fail more often despite contrary objective data) is termed confirmation bias,” Dr Renouard explains. “This type of bias is a very common cognitive behavior: Once a decision has been made or a ‘fact’ learned, the human brain will always look for data that corroborate the preconceived notion in question and dismiss data challenging these notions. It is an unfortunate but frequent occurrence in many scientific fields.”
Current Knowledge
With the problems present in early research on short implants, where does the current literature stand? Dr Deporter’s book Short and Ultra-Short Implants provides a valuable update.
Some short implant designs have proven to be a legitimate substitute for longer implants used in conjunction with a dedicated open sinus floor elevation and grafting procedure.

For this patient, short implants were used to retain a mandibular overdenture. Four 7-mm-long Brånemark-type implants were allowed submerged healing and subsequently connected with a customized bar structure. (a) Intraoral view at the 15-year recall of a patient’s four 7-mm-long implants and connecting bar. The peri-implant soft tissues appear healthy. (b) Radiograph at the 15-year recall. Peri-implant bone levels appear stable.
While these may seem like specific indications, experienced clinicians will recognize that no implant size or length can feasibly be used as a one-size-fits-all solution. Short and ultra-short implants therefore represent a valuable treatment option for situations that would generally require invasive augmentative procedures in order to place standard-length implants. Short implants also present several advantages, including lower risk of neurovascular damage in the posterior mandible, lower risk of sinus damage or infection in the posterior maxilla, simpler and less invasive surgical procedures, shorter treatment times, higher patient acceptance, and lower treatment costs for the patient. Even so, many clinicians may still feel more comfortable placing standard-length implants in conjunction with adjunctive surgical procedures, even in situations where short implants have proven successful. In the book, Dr Deporter and his colleagues address some of the common concerns that prevent clinicians from using short implants.
No implant size or length can feasibly be used as a one-size-fits-all solution.
Another concern is the fact that short implants cannot be treated the same as standard-length implants. Rather, a successful outcome largely depends on the clinician’s ability to correctly modify surgical protocols when placing short implants.
“Clinical data has shown that outcomes could be significantly improved by modifying standard threaded implant osteotomy preparation techniques,” Dr Deporter explains. “Preoperative evaluation of bone quality and density using CBCT can help the surgeon determine which modifications to make, which may include modified approaches such as an undersized osteotomy or a stepped osteotomy.”

(a) This patient was first treated with vertical ridge augmentation followed by placement of standard-length threaded implants and fixed prostheses. These later failed with loss of the grafted bone. (b) The patient was re-treated using two 4 × 4.5–mm self-tapping moderately rough threaded implants in the right mandible and two 4 × 4–mm self-tapping moderately rough threaded implants in the left mandible (all Global D implants). After removing the failed implants seen in a and without further bone grafting at the patient’s request, the sites were allowed to heal for 4 months before the ultra-short implants were placed. This radiograph was taken 1 year after the retreatment was completed. (c) This radiograph shows the right-side restoration after 4 years in function. (d) This radiograph shows the left-side restoration after 4 years in function.

(a) Treatment for this patient began with a vertical bone augmentation procedure. This procedure was unsuccessful, so the plan was changed to use three ultra-short 4 × 4–mm self-tapping moderately rough threaded implants. (b) A definitive prosthesis on its master cast. Note the accuracy and the polishing of the metal substructure to discourage dental plaque accumulation. (Courtesy of Dr Fabio Colombelli, Milan, Italy.) (c) A radiograph of the definitive prosthesis in place. (d) The clinical design of the definitive prosthesis showing optimal access for oral hygiene.

(a) Two single SPSIs were used to replace the maxillary right first premolar and first molar. The premolar site has a 7 × 4.1–mm (6-mm DIL) implant, while a 5 × 5–mm (4-mm DIL) implant was chosen for the molar site to avoid the need for a dedicated indirect sinus floor elevation procedure. Both implants (OT-F3) have an incorporated platform-switch feature. (b) Single anatomically correct metal-ceramic crowns were used for the two implants. (Restorations provided by Dr Ester Canton, Toronto, Ontario.)

(a) An ultra-short 5 × 4.1–mm (4-mm DIL) SPSI (Endopore) was placed in 3 mm of subantral bone using bone-added osteotome sinus floor elevation. A major portion of the implant length sits in new bone that formed following the sinus grafting. (b) A CBCT scan of the implant after 6 months of submerged healing prior to reentry and restoration. The majority of the implant is surrounded by new bone at this time. (Restoration by Dr Jeffrey Reynolds, Toronto, Ontario.)
Changing Perspectives
For the periodontist who has dedicated his career to the research and development of short implants, the changes occurring today are better late than never.
“Progress in dentistry is generally slow when it comes to applying research data to routine clinical practice,” Dr Deporter explains, “but it feels good to see change happening even if it has been at a snail’s pace. I have always felt that short would triumph in the long term, particularly when colleagues in countries other than the US started replicating and expanding upon our findings with SPS implants. Unfortunately, however, many dental practitioners—particularly in North America—still look to industry for answers rather than seeking out published independent research data. Luckily, most implant manufacturers have now seen the light and begun to produce short implant models, some as short as 4 mm. The fact that so many companies now produce short implants is a clear indication that there is a perceived high demand for them.”
However, there is also the potential to move backward and lose the ground so painstakingly gained. “I can only hope,” Dr Deporter says, “that any manufacturer that provides short implant options will have sufficient clinical trial data beforehand to provide defined proper protocols and limitations specific to their offerings. Short implants can be successful, but only if protocols are strictly followed and if clinicians pursue adequate information before using them. My fear is that the progress made to date may be undermined by high failure rates from clinicians who fail to understand that shorter does not necessarily mean simpler.
“Did I ever waver in my belief that short was good?” he continues. “That’s easy to answer: No. As they say, the proof is in the pudding.”
 Douglas Deporter, DDS, Dip Perio, PhD, has been a full-time member of the Faculty of Dentistry at the University of Toronto since 1976. He has been involved in clinical research in implant dentistry for over 30 years and has published extensively on short and ultra-short implants, particularly those with sintered porous-surfaced (SPS) topography. He was coinventor of the original SPS implant (Endopore), the patent for which was assigned to the University of Toronto. Dr Deporter has given more than 140 invited international presentations. He also maintains a part-time private practice limited to periodontics and implant dentistry in Toronto, Ontario.
Douglas Deporter, DDS, Dip Perio, PhD, has been a full-time member of the Faculty of Dentistry at the University of Toronto since 1976. He has been involved in clinical research in implant dentistry for over 30 years and has published extensively on short and ultra-short implants, particularly those with sintered porous-surfaced (SPS) topography. He was coinventor of the original SPS implant (Endopore), the patent for which was assigned to the University of Toronto. Dr Deporter has given more than 140 invited international presentations. He also maintains a part-time private practice limited to periodontics and implant dentistry in Toronto, Ontario.
 Short and Ultra-Short Implants
Short and Ultra-Short Implants
Edited by Douglas Deporter
Research has shown that short implants are not only a viable option but oftentimes a superior one that carries fewer risks for the patient and dentist, especially in resorbed jaw sites. As clinical trials continue to underscore the safety and efficacy of short implants, more dentists are considering their use with real interest, and this book provides the information clinicians need to incorporate short implants into their own practice. The book reviews the clinical effectiveness of short implants and then describes treatment protocols for the various types of short implants and their placement in different areas of the mouth. Case presentations demonstrate the recommended techniques and showcase the results.
168 pp (softcover); 334 illus; ©2018; ISBN 978-0-86715-785-7 (B7857); US $85