Cleared specimens of maxillary first molar mesiobuccal roots showing the complex canal anatomy and endodontic treatment task. (Courtesy of Dr Craig Barrington, Waxahachie, Texas.)
Dr Noah Chivian first argued for the conservative nature of surgical endodontics in a 1969 article in the Journal of the New Jersey Dental Association titled “Surgical Endodontics, A Conservative Approach”; it is now 2017, and the industry continues to have this debate.
“Conservative is commonly defined as ‘disposed to preserving existing conditions,'” Dr Chivian explains, reflecting on his 1969 article. “At that time, popular dental semantics referred to the two courses of endodontic action as conservative and surgical. This implies that the surgical approach is radical and the nonsurgical approach is conservative. However, both of these methods try to ‘preserve existing conditions’ by retaining teeth, and therefore both must be considered conservative. In fact, modern endodontic surgery may be more conservative than disassembly, retreatment, and re-restoration.”
Two acclaimed endodontists, Mahmoud Torabinejad, DDS, MSD, PhD, and Richard Rubinstein, DDS, MS, hope to settle this argument for good with their new book, The Art and Science of Contemporary Surgical Endodontics.
“Endodontic surgery is inherently conservative because it is an alternative to tooth extraction, a radical and aggressive treatment that results in the loss of an organ, in many cases,” Dr Torabinejad states.
“The current paradigm being taught in most residencies is that if an endodontic treatment fails, retreatment must be performed or attempted before endodontic surgery can be considered,” Dr Rubinstein says. “But in complex cases involving posts and cores, sometimes the disassembly required for retreatment compromises too much tooth structure, and extraction becomes inevitable. This is the opposite of conservative.”
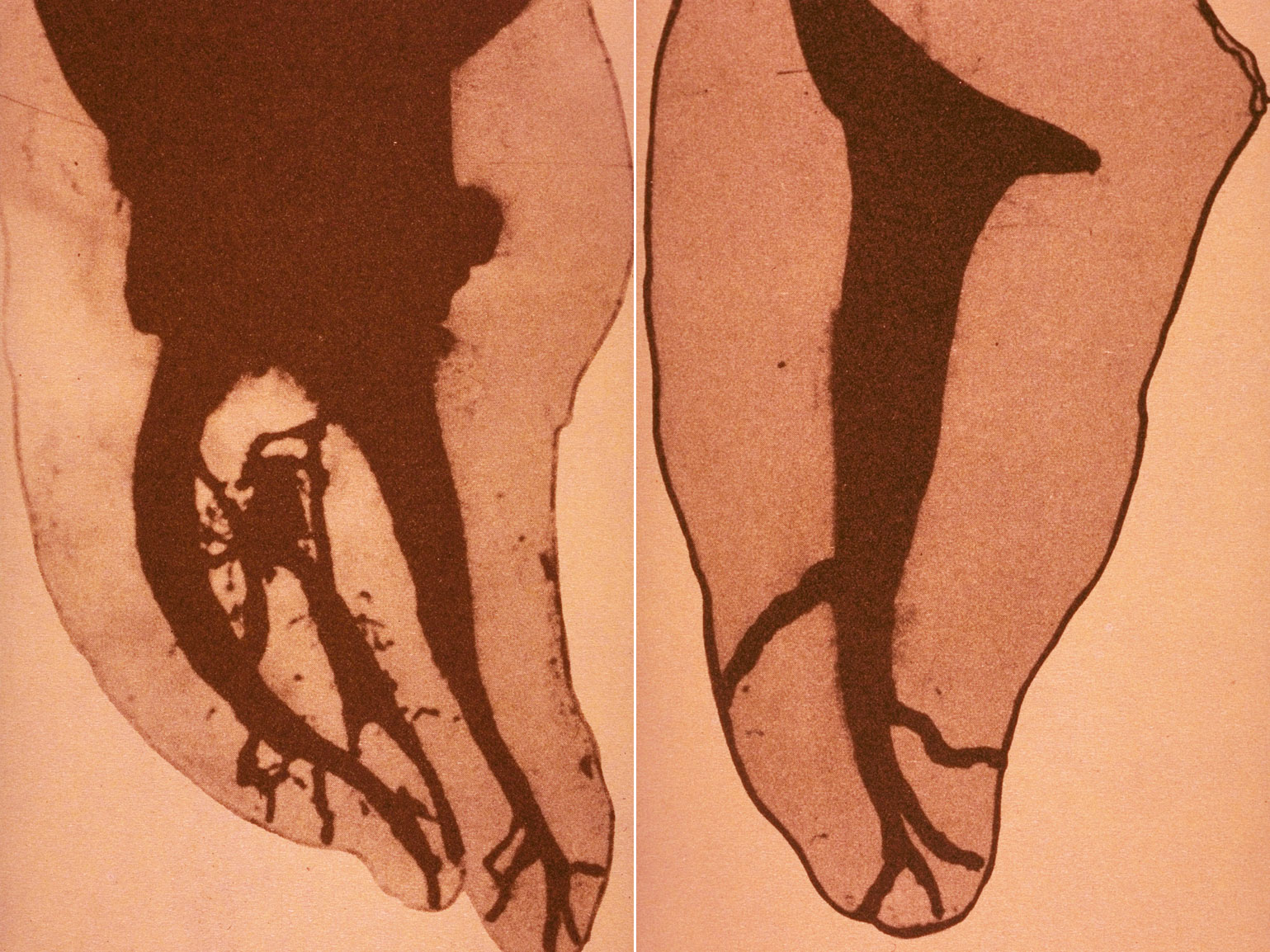
(left) Hess model of a mandibular molar showing anatomical complexities throughout the root canal system. (right) Hess model of a mandibular premolar showing anatomical complexities in the apical terminus.
Modern Advances in Surgical Endodontics: Possibility Becomes Predictability
According to Dr Rubinstein, there is a difference between possibility and predictability. And the point when endodontic surgery became more predictable—and therefore more conservative—than retreatment for complex cases came when modern technology, namely cone beam computed technology (CBCT) and surgical operating microscopes (SOMs), enabled endodontic surgeons to better identify and more accurately treat complex tooth morphologies.
The incidence of anatomical complexities in root canals is well documented. CBCT technology enables clinicians to identify these complexities and plan for them. “Failure to address these complexities,” Dr Rubinstein asserts, “leaves the tooth vulnerable to reinfection. Significant pulpal anatomy such as accessory canals and isthmi has to be considered when performing both surgical and nonsurgical endodontic treatment.”

Doctor and assistant at the SOM.
The SOM made it possible to manage those complexities during surgery. Dr Rubinstein was one of a handful of endodontists who first began experimenting with the SOM for apical surgery: “We thought, ‘If you can see something better, you can treat it better,’ and the results were overwhelming. Cases that seemed impossible before became easy and exciting to operate on, and teeth that might otherwise have been extracted now had a predictable chance for retention.”
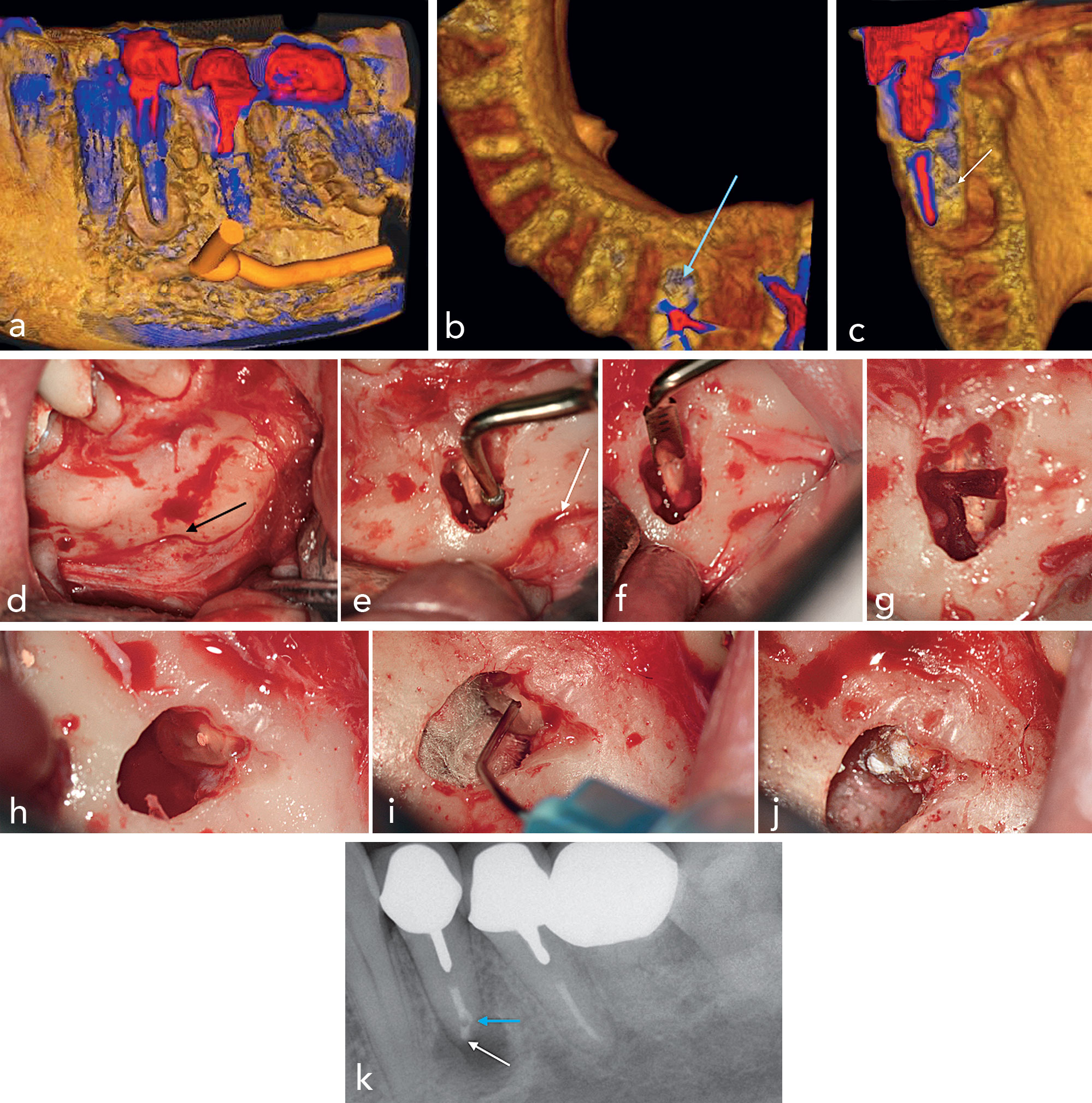
(a) 3D rendering of the mandibular left first premolar showing the periapical lesion and its relationship to the mental bundle. (b and c) Axial and coronal 3D renderings showing the untreated lingual canal (blue and white arrows), the extent of the lesion buccolingually, and the relationship of the root to the buccal and lingual cortical plates (c). (d) Clinical image after flap reflection and identification of the mental bundle (black arrow). (e) Because of the close proximity of the root to the mental bundle (white arrow), a piezoelectric surgery insert OT5 (Mectron) was used for the osteotomy. (f) Root resection performed with OT7S-3 insert (Mectron). (g) Resected apical third with the OT7S-3 insert. (h) Clinical image demonstrating the untreated lingual canal (white arrow) and isthmus. (i) Application of EndoSequence BC Sealer (Brasseler USA) into the apical preparation prior to placement of the Root Repair Material (RRM) (Brasseler USA). (j) RRM material filling in the buccal and lingual canals. (k) Postoperative radiograph demonstrating the RRM filling in the lingual canal (white arrow) and buccal canal (blue arrow).
Changing the Paradigm
There are many reasons why endodontic surgery is not as popular as nonsurgical endodontics or implant dentistry, but the biggest obstacle to wider implementation is education-based.
“There is just not enough time in an endodontic residency to teach surgery,” Dr Torabinejad laments. “If the endodontist isn’t adequately trained in endodontic surgery, they may refer the patient to an oral surgeon who also may not be adequately trained, resulting in the extractions of teeth that could have been saved.”
The shortage of residencies that train students in endodontic surgery also means there is a shortage of teachers, but Drs Torabinejad and Rubinstein hope their textbook will help bridge these gaps. “Our book covers endodontic surgery and the rationale behind it from A to Z,” Dr Torabinejad explains, “and the surgical videos included with the book will allow readers to see how endodontic surgeries are performed so they will be more comfortable performing them.”
In an era where dental implants are widely used and generally successful, it may not seem especially detrimental to extract a compromised tooth and replace it with an implant. However, a recent survey by the American Association of Endodontists found that patients have strong opinions favoring the retention of their natural teeth. According to the survey, most participants were not aware that root canal treatment is a viable alternative to tooth extraction, but 76% of participants would prefer to have a root canal than a tooth extraction. From these results, it can be inferred that patients prefer the most conservative approach—both medically speaking and financially. And that should be enough to inspire clinicians to broaden their repertoire.
“I was presenting at a conference,” Dr Rubinstein recalls, “and we were asked, ‘What do you think makes a specialist a specialist?’ I said, ‘Our willingness to take risks for our patients.’ Afterward, someone came up to me and said he took great offense at my implying he doesn’t take risks for his patients because he doesn’t perform surgery. So I asked him if he thought he would be more open to endodontic surgery if he’d had training for it in his residency, and he said maybe. He came back to me before the end of that conference and said he thought I may be right and asked if I had any recommendations for workshops he could take. There is a personal comfort level that we as clinicians have to push past so we can better serve our patients.”
 The Art and Science of Contemporary Surgical Endodontics is an excellent start to meeting that educational need, and the authors hope it will serve as a catalyst for educators and clinicians to rethink the way they define conservative endodontic treatment and as a learning tool for those eager to broaden their horizons.
The Art and Science of Contemporary Surgical Endodontics is an excellent start to meeting that educational need, and the authors hope it will serve as a catalyst for educators and clinicians to rethink the way they define conservative endodontic treatment and as a learning tool for those eager to broaden their horizons.
 Mahmoud Torabinejad, DDS, MSD, PhD, is a professor of endodontics and director of the advanced specialty education program in endodontics at Loma Linda University School of Dentistry. He has made over 200 national and international presentations in more than 40 countries, has authored four textbooks and more than 300 publications, and is the top-cited author in endodontic journals with authorship in 16 articles of the top 100 list. He has received numerous awards and accolades, including the Edward D. Coolidge Award from the AAE in 2016 for displaying leadership and dedication to dentistry and endodontics. He is past president of the California Association of Endodontics and past president of the American Association of Endodontists and its Foundation.
Mahmoud Torabinejad, DDS, MSD, PhD, is a professor of endodontics and director of the advanced specialty education program in endodontics at Loma Linda University School of Dentistry. He has made over 200 national and international presentations in more than 40 countries, has authored four textbooks and more than 300 publications, and is the top-cited author in endodontic journals with authorship in 16 articles of the top 100 list. He has received numerous awards and accolades, including the Edward D. Coolidge Award from the AAE in 2016 for displaying leadership and dedication to dentistry and endodontics. He is past president of the California Association of Endodontics and past president of the American Association of Endodontists and its Foundation.
 Richard Rubinstein, DDS, MS, received his dental degree in 1971 and his endodontic training in 1973, both from the University of Michigan School of Dentistry, where he is currently an adjunct clinical professor in the Department of Cariology, Restorative Sciences and Endodontics. He is an internationally renowned speaker and pioneer in the use of the operating microscope in endodontics. In addition to writing numerous scientific articles on the surgical operating microscope and endodontic microsurgical technique, he is a contributing author of several endodontics textbooks. He is a Fellow of the American College of Dentists and maintains a private practice limited to endodontics in Farmington Hills, Michigan.
Richard Rubinstein, DDS, MS, received his dental degree in 1971 and his endodontic training in 1973, both from the University of Michigan School of Dentistry, where he is currently an adjunct clinical professor in the Department of Cariology, Restorative Sciences and Endodontics. He is an internationally renowned speaker and pioneer in the use of the operating microscope in endodontics. In addition to writing numerous scientific articles on the surgical operating microscope and endodontic microsurgical technique, he is a contributing author of several endodontics textbooks. He is a Fellow of the American College of Dentists and maintains a private practice limited to endodontics in Farmington Hills, Michigan.